
Hypertension is the most important treatable risk factor worldwide and goes along with 214 million DALYs (= disability-adjusted life-years = years of life lost [YLLs] plus years lived with disability [YLDs]) due to i. e. ischaemic heart disease and stroke [GBD 2016 Risk Factors Collaborators 2017]. The prevalence of arterial hypertension worldwide is estimated to be 626 million in women and 652 million in men aged 30 to 79 years with detection rates of 59 % and 49 %, treatment rates of 47 % and 38 %, and control rates of 23 % and 18 % in women and men, respectively [NCD-RisC 2021].
Summary
Introduction: Hypertension guidelines emphasise patient education for efficient implementation of non-pharmacological and pharmacological therapy. Structured hypertension education programmes (HEPs) have been developed to improve the efficacy of hypertension treatment with varying efficacy. The German Society of Hypertension DHL developed a modular interactive group training programme in the primary care setting.Methods: This study aims to test the blood pressure (BP) lowering efficacy of this hypertension education programme versus usual care in patients with mild arterial hypertension in primary care. In an open-label cluster-randomised design, patients from eight primary healthcare practices were included in the study (35 patients from 4 practices in the intervention group, and 53 patients from other 4 practices in the control group completed the study).
Results: Patients were followed six months, and the primary endpoint was office systolic BP. In the intervention group, the reduction in systolic office BP was significantly greater (by 8 mmHg, p < 0.05) than in the control group. Moreover, significantly greater reductions in diastolic office BP (by 5 mmHg), systolic home BP (by 9 mmHg) and in diastolic home BP (by 6 mmHg) were achieved in the intervention group as compared to the control group (each p < 0.05, respectively, secondary endpoints).
Conclusions: The participation in the hypertension education programme of the German Hypertension Society was associated with significant reductions in office and home BP after six months in patients with mild arterial hypertension. This programme may therefore provide an efficient tool for hypertension management in the primary health care setting.
Key words
clinical management of high blood pressure, non-pharmacological therapy, patient education, primary care issues, outcomes of care
Wirksamkeit des Schulungsprogramms der Deutschen Hochdruckliga DHL (MEIN BLUTDRUCK – OK!)
Zusammenfassung
Einleitung: Leitlinien zu Bluthochdruck (blood pressure, BP) legen für eine effiziente Umsetzung der Therapie Wert auf die Patientenschulung. Die Deutsche Hochdruckliga (DHL) hat ein modulares, interaktives Gruppenschulungsprogramm für die Primärversorgung entwickelt.
Methoden: Ziel dieser Studie ist es, die blutdrucksenkende Wirksamkeit des Schulungsprogramms im Vergleich zur Standardversorgung bei Patienten mit leichter arterieller Hypertonie in der Primärversorgung zu untersuchen. In einem offenen, cluster-randomisierten Design wurden Patienten aus acht Hausarztpraxen untersucht (Intervention n = 35, Kontrolle n = 53).
Ergebnisse: In der Interventionsgruppe war die Senkung des systolischen BP in der Praxis nach sechs Monaten (primärer Endpunkt) signifikant größer (8 mmHg, p < 0,05) als in der Kontrollgruppe. Zudem wurden signifikant stärkere Senkungen des diastolischen BPs in der Praxis (5 mmHg), des systolischen BPs zu Hause (9 mmHg) und des diastolischen BPs zu Hause (6 mmHg) erzielt (jeweils p < 0,05).
Schlussfolgerungen: Die Teilnahme am Schulungsprogramm der DHL führte bei Patienten mit leichter arterieller Hypertonie nach sechs Monaten zu einer signifikanten Senkung des Blutdrucks. Das Programm könnte ein wirksames Instrument für das Bluthochdruckmanagement in der primären Versorgung sein.
Schlüsselwörter
klinisches Management von Bluthochdruck, nichtmedikamentöse Therapie, Patientenschulung, Fragen der Primärversorgung, Behandlungsergebnisse
Introduction
In high-income Western countries detection rates were 73 % and 69 %, treatment rates were 64 % and 58 %, and control rates were 43 % and 37 % in women and men, respectively [NCD-RisC 2021]. Accordingly, hypertension prevalence is also high in Germany with about 20 million adults aged 18 to 79 years (30 % in women, 33 % in men) being affected [Neuhauser 2013]. Hypertension awareness has been increasing between 1998 and 2008 from 69 % to 82 % (women 74 % to 87 %, men 65 % to 78 %) as has hypertension control (practice measurement < 140/90 mmHg) from 23 % to 51 % (women 25 % to 58 %, men 20 % to 45 %) [Neuhauser 2015]. Guidelines from European and US hypertension societies suggest that lifestyle changes should be implemented in all stages of hypertension as well as with high-normal blood pressure (BP), and furthermore that nonadherence is a major risk factor for insufficient blood pressure control in up to 50 % of patients [Mancia 2023, McEvoy 2024, Jones 2025]. To successfully implement lifestyle changes and tackle nonadherence, hypertension education programmes (HEPs) have been developed in several countries worldwide. The Canadian Hypertension Education Programme (CHEP) is an unique Canadian initiative to improve awareness, treatment and control of hypertension through the education of health care professionals [Feldman 2008]. Between 1996 and 2003, there was a 65.1 % increase in the number of individuals diagnosed with hypertension (from 2.7 million in 1996 to 4.4 million in 2003) and a 77.0 % increase in the number of individuals being treated with antihypertensive drugs for hypertension in Canada [Campbell 2009]. There were significant reductions (p < 0.0001) in the rate of death from stroke, heart failure, and myocardial infarction starting in 1999. The changes in mortality (p < 0.001 for all three diseases) and hospitalization (p < 0.0001 for stroke and heart failure; p = 0.018 for acute myocardial infarction) were associated with the increases in antihypertensive prescriptions, coinciding with the introduction of CHEP. The CHEP educational model for improving health care could be adopted by other countries [Campbell 2009]. Other educational programmes have been implemented in several countries e. g. The National High Blood Pressure Education Program (NHBPEP) has been started already in 1973 in the US with a focus on "translation of scientific studies into practical and useful education programmes that would increase awareness about the benefits of treating hypertension and motivate the American people, physicians, nurses, pharmacists, and public health workers to do a better job of managing this disease" [Cziraky 2002], and in Finland an education and information programme focusing on salt intake has proven to be very successful [Moser 2013, Vartiainen 1991]. In Germany, local hypertension education programmes in Mecklenburg-Vorpommern/North-Rhine-Westphalia using four 90 to120 minutes sessions dealing with BP self-measurement, diet, antihypertensives, and risk factors/need for follow-up examinations and in Bavaria using eight 90 minutes sessions dealing with the achievement of better blood pressure control, the reduction of other concomitant cardiovascular risk factors, the strengthening of beneficial health-related behaviour and education of blood pressure self-measurement as well nonpharmacological strategies to lower blood pressure have already been developed and reported initially in 1997 and 2000 [Gruesser 1997, Mühlhauser 1993, Danzer 2000, Fleischmann 2004]. These programmes have shown some improvement in blood pressure control and were associated with a slight weight loss. We present the results of implementation of a more intensive and comprehensive five-day hypertension education and training programme sponsored by the German Society of Hypertension (Deutsche Hochdruckliga, DHL), MEIN BLUTDRUCK – OK!, and intended for nationwide use.
BMI: body mass index
BP: blood pressure
CHEP: Canadian Hypertension Education Programmee
GFR: estimated glomerular filtration rate
HDL: high density lipoprotein
HEP: hypertension education programme
LDL: low density lipoprotein
Methods
Design and Setting
Patients with mild arterial hypertension, at least 22 years old, with regular survey in primary healthcare practices, were enrolled in the study. The study enrolled a total of eight primary healthcare practices for participation in the study. These outpatient clinics were cluster randomised either to regular care or to the application of the hypertension education programme of the German Hypertension Society (MEIN BLUTDRUCK – OK!) to the patients. In these primary healthcare clinics, all included patients received either the hypertension education programme or usual care. Clinics randomised to usual care offered their patients the hypertension education programme after the follow-up (thus after six months). It was deemed not possible to offer patient level randomisation to the hypertension education programme and usual care in each primary care practice, a drop out from usual care and spill-over to the education programme would have been the likely consequence.
Only stable preferably untreated patients with essential hypertension were chosen who were not likely to need to change antihypertensive medication within six months. For inclusion, patients had to have office blood pressure measured between 140/90 mmHg and 159/99 mmHg.
Exclusion criteria were unstable clinical condition, secondary arterial hypertension, dementia, major disability (modified Ranking-Scale > 4), severe chronic kidney disease (serum creatinine > 2 mg/dl or estimated glomerular filtration rate (eGFR) < 40 ml/min/1.73 m2 body surface), liver disease including history of hepatic encephalopathy, esophageal varices or portocaval shunt, history of gastrointestinal operation or disease with a potential influence on drug absorption, allergies or contraindications against antihypertensive drugs, history of non-adherence and participation in another clinical trial.
The hypertension education programme of the German Hypertension Society (MEIN BLUTDRUCK – OK!) is an interactive modular group training programme [Eckert 2015]. Patients are trained preferentially by clinic staff (hypertension assistants qualified by the German Hypertension Academy), else by physicians. In small groups of four to six patients, they receive education in five distinct sessions. Each ad session takes about two hours. With each session, patients receive a booklet with information relevant to the session. All five sessions were completed within three months. The scope of the five educational sessions were blood pressure regulation, causes of hypertension, target blood pressure, hypertension diagnostics (module 1), non-pharmacological interventions for hypertension one (lifestyle, diet, exercise; module 2), non-pharmacological interventions for hypertension two (relaxation techniques, instructions for hypertensive urgencies and emergencies, blood pressure self-measurement; module 3), pharmacological treatment of hypertension (module 4) and adherence (regular drug intake, hypertension support groups, telemedicine; module 5).
Patients were included into the study if they fulfilled the inclusion and exclusion criteria and informed consent was obtained. Patients in the usual care group (control clinics) received general verbal advice by their physicians.
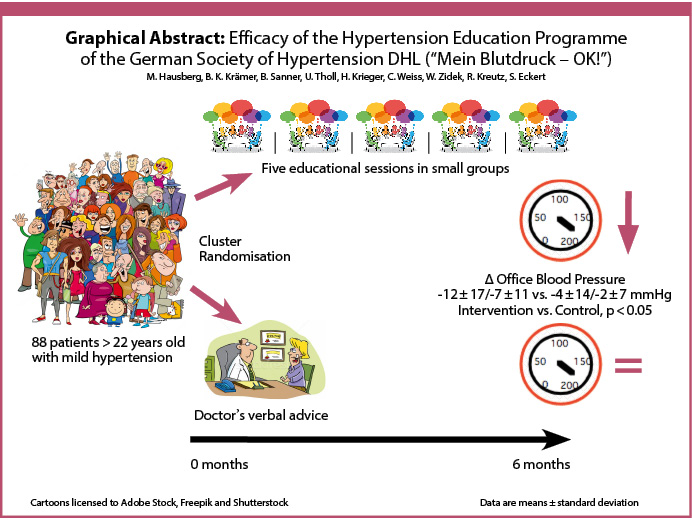 Abb: Graphical Abstract
Abb: Graphical Abstract
Assessments
After inclusion into the study, a baseline visit was performed. Sitting office blood pressure was measured in a standardised way as described elsewhere [Eckert 2019], using an automated upper arm oscillometric sphygmomanometer. Height and weight were measured, body mass index (BMI) calculated and blood samples taken for analysis of serum creatinine, estimated glomerular filtration rate (Modification of Diet in Renal Disease (MDRD) formula), uric acid, glycosylated haemoglobin (HbA1c), total, high density lipoprotein (HDL)- and low density lipoprotein (LDL)-cholesterol and triglycerides.
Patients were provided with a certified upper-arm oscillometric sphygmomanometer (if they did not already have one) and instructed for standardised home blood pressure measurements as described elsewhere [Eckert 2019]. Home blood pressure was recorded during the week after the baseline visit.
Also, ambulatory blood pressure monitoring (ABPM) was performed within one week of the baseline visit, where available.
Moreover, patients received a multiple-choice questionnaire. Patients were asked to describe subjective health perception, limitations in physical activity, limitations at work, limitations in contacts with family and friends, pain perception and emotional well-being. These questions were taken from the Short Form Health Survey SF-12 [Côté 2004]. Patients were also asked to answer questions concerning the diagnosis and management of hypertension (subject of the hypertension education programme). Moreover, they had to indicate the amounts of physical activity and alcohol consumption.
In the intervention group, the hypertension education modules started within two weeks after the baseline visit.
If a patient needed a change in his antihypertensive medication during the study period (six months) the patient was excluded from the study.
Six months after the baseline visit a final visit was performed, the same parameters were measured as with the baseline visit. Home blood pressure measurements were again recorded during the week before the final visit, and another ambulatory blood pressure monitoring was taken within two weeks around the final visit, where available. Patients again received the multiple-choice questionnaire described above.
The primary endpoint was the change in systolic office blood pressure from baseline to six months. An at least 5 mmHg greater reduction of systolic office blood pressure in the intervention group was deemed to prove clinically relevant efficacy. Secondary endpoints were changes in diastolic office blood pressure from baseline to six months, changes in systolic and diastolic home blood pressures from baseline to six months, the changes in ABPM daytime mean systolic and diastolic blood pressures, changes in body mass index from baseline to six months and changes in the above specified laboratory parameters from baseline to six months and finally changes in self reported parameters described above.
Statistical analysis
Data collection and monitoring was performed by signum [ pr health communication GmbH, Im Medipark 5c, D-50670 Köln, Germany.
Based on previous studies, a decrease in systolic office blood pressure by 8 mmHg could be expected with a hypertension education programme as compared to usual care [Gruesser 1997, Kurz 2005]. The estimated standard deviation of office systolic blood pressure was 12 mmHg.
With respect to the cluster randomisation design, we expected an intra-cluster correlation coefficient of 0.01 and thus with eight clusters with a cluster size of ten to twelve a design effect of about 1.07. Thus for an alpha error of 0.05 and a beta error of 0.20 a sample size of 39 for each group was estimated [Kerry 1998]. We expected a total of 80 patients available for analysis based on the expected inclusion of at least 100 patients and considering a drop-out rate of 20 %.
For the comparison of two independent groups regarding a categorial factor (i. e. sex), Chi2 test has been performed. For quantitative variables approximately normally distributed (i. e. blood pressure variables), a 2 sample t test has been used. If a normal distribution could not be assumed (i. e. subjective health parameters), a Wilcoxon 2 sample test has been applied. To evaluate changes over time regarding blood pressure values or laboratory parameters and to test for interactions between group and time, repeated measures analysis of variance has been performed with group and time as fixed factors and patients’ ID as a random factor.
Quantitative data are reported as mean plus standard deviation (std). Furthermore, 95 % confidence intervals for the mean difference of the changes in blood pressure have been calculated. For the health parameters, median values are presented. For qualitative factors, absolute and relative frequencies are given.
Statistical analysis was performed using Statview 5.0.1 for MacOS, Abacus corporation, or SAS, release 9.4 (SAS Institute Inc., Cary NC 27513, USA).
The study was performed according to good clinical practice and the declaration of Helsinki. The study design was approved by the ethics committee of the Ruhr University of Bochum, Germany, identifier no. AZ 25/2915. Written informed consent was obtained from all study participants. The study was registered at ClinicalTrials.gov, identifier: NCT02676414, "Validation of a Hypertension Education Program".
Results
Eight primary care outpatient clinics could be recruited for participation in the study, these practices are listed in the acknowledgments.
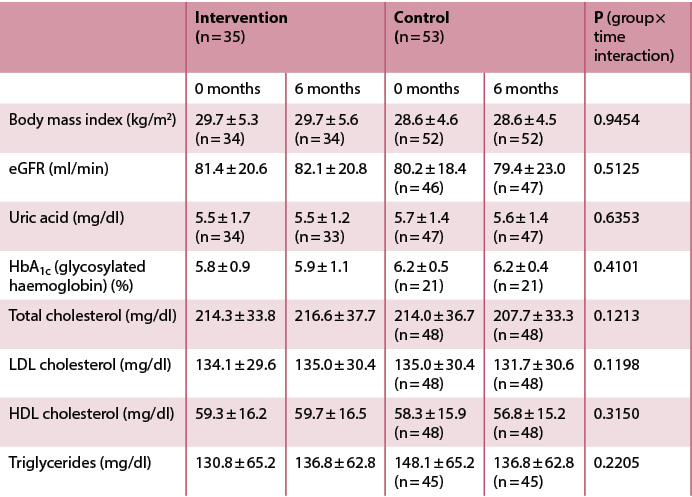
A total of 88 patients completed the study between 2015 and 2017 and were available for analysis. Four primary care outpatient clinics were randomised to the intervention group (hypertension education programme) – 40 patients were included of whom 35 completed this study arm. Four primary care outpatient clinics were randomised to usual care – 76 patients were included of whom 53 completed that study arm. Results are reported only for patients who completed the study. Baseline data are presented in table 1.
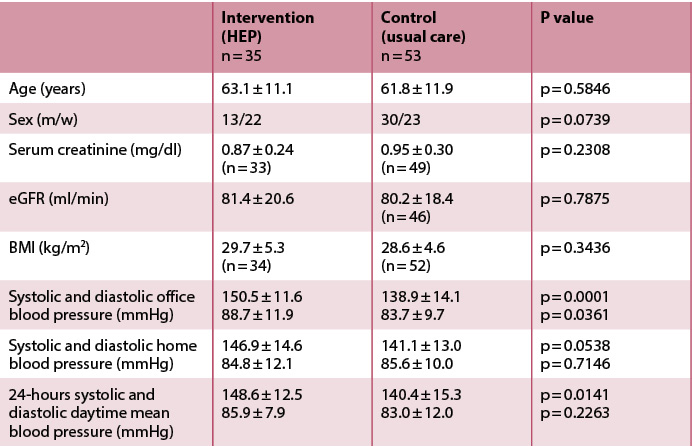 Tab. 1: Baseline characteristics of the intervention and control groups, quantitative data are given as mean ± standard deviation.
Tab. 1: Baseline characteristics of the intervention and control groups, quantitative data are given as mean ± standard deviation.
From the baseline visit to the six months visit, systolic office blood pressure decreased by 12 ± 17 mmHg vs. 4 ± 13 mmHg in the intervention and control group, respectively (p = 0.0111). The primary endpoint was reached. There were also significantly greater reductions in diastolic office blood pressure (p = 0.0127) and in systolic and diastolic home blood pressure in the intervention vs. control group (p = 0.0054 and p = 0.0122, respectively). For 24-hours daytime mean blood pressure reductions no statistically significant differences between intervention and control group were observed (1.2 mmHg and 3.5 mmHg greater reductions in ABPM daytime means for systolic and diastolic blood pressure in the intervention vs. control groups, n. s.), cf. table 2 and figures 1, 2.
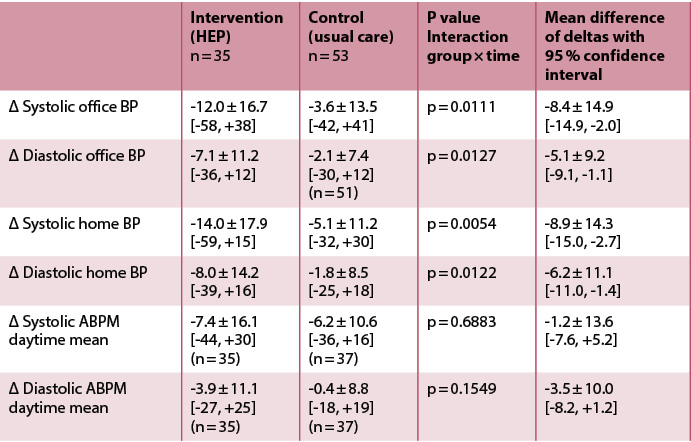 Tab. 2: Change in blood pressure values in the intervention and control groups 6 months after inclusion vs. baseline (in mmHg, quantitative data are given as mean ± standard deviation together with their range).
Tab. 2: Change in blood pressure values in the intervention and control groups 6 months after inclusion vs. baseline (in mmHg, quantitative data are given as mean ± standard deviation together with their range).
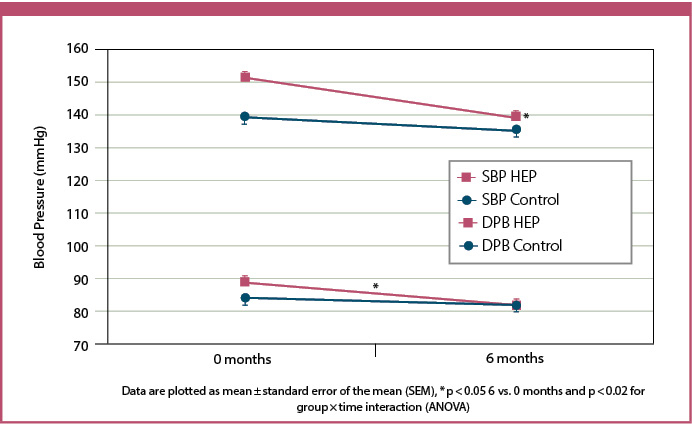 Fig. 1: Office blood pressure in the intervention (hypertension education programme = HEP; n = 35) and control (n = 53) groups; SBP = systolic blood pressure, DPB = diastolic blood pressure.
Fig. 1: Office blood pressure in the intervention (hypertension education programme = HEP; n = 35) and control (n = 53) groups; SBP = systolic blood pressure, DPB = diastolic blood pressure.
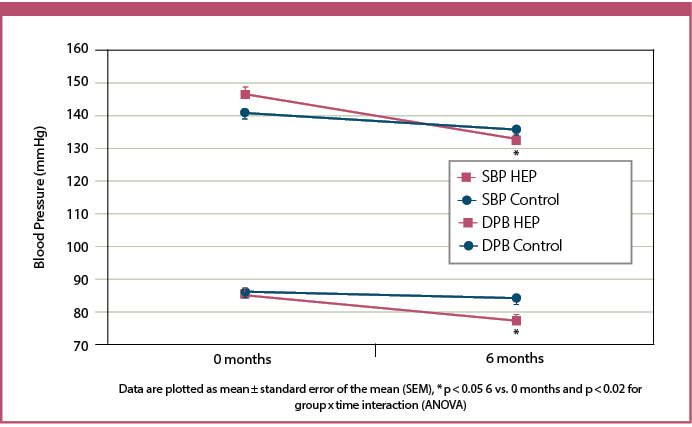 Fig. 2: Home blood pressure in the intervention (hypertension education programme = HEP; n = 35) and control (n = 53) groups; SBP = systolic blood pressure, DPB = diastolic blood pressure.
Fig. 2: Home blood pressure in the intervention (hypertension education programme = HEP; n = 35) and control (n = 53) groups; SBP = systolic blood pressure, DPB = diastolic blood pressure.
As far as the other secondary endpoints are concerned, there were no statistically significant changes in body weight, body mass index, serum creatinine, estimated glomerular filtration rate, total cholesterol, LDL-cholesterol, HDL-cholesterol or triglycerides in either group., cf. table 3a. No interaction between group and time could be observed either.
 Tab. 3a: Body mass index, laboratory parameters and patient reported subjective health parameters at baseline and after 6 months in the intervention and control groups, data are mean±standard deviation.
Tab. 3a: Body mass index, laboratory parameters and patient reported subjective health parameters at baseline and after 6 months in the intervention and control groups, data are mean±standard deviation.
As far as patient reported data are concerned (cf. table 3b), fitness for strenuous activities (climbing multiple stairs) appeared to increase in the intervention group but not in the control group (p = 0.0010). Subjective pain perception decreased in the intervention but not in the control group (p = 0.0547).
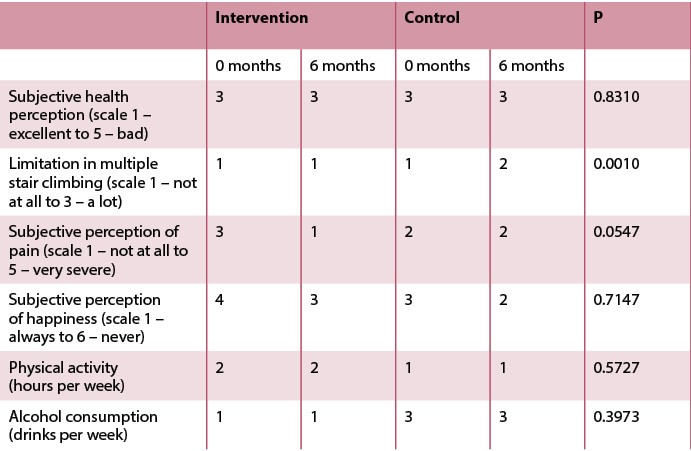 Tab. 3b: Patient reported subjective health parameters at baseline and after 6 months in the intervention and control groups, data are median, p values for the comparison of the changes in the intervention and control groups (derived by Wilcoxon 2 sample tests).
Tab. 3b: Patient reported subjective health parameters at baseline and after 6 months in the intervention and control groups, data are median, p values for the comparison of the changes in the intervention and control groups (derived by Wilcoxon 2 sample tests).
Subjective perception of overall health, of happiness and other emotional parameters, subjective limitations in moderate or easy activities and subjective limitations at work were not significantly different between groups and did not change significantly over time.
Patient reported physical activity and alcohol consumption also were not significantly different between groups and did not change significantly over time.
Concerning the questions about hypertension diagnosis and management, between one third and all of patients provided correct answers, depending on the difficulty of the questions. However, there were no significant differences between groups and no significant changes over time – except for one difficult question concerning Jacobson progressive muscle relaxation, where a greater proportion of patients in the intervention group indicated the correct answer after six months than at baseline. The other data are not shown.
Discussion
The participants in the hypertension education programme MEIN BLUTDRUCK – OK! of the German Hypertension Society [Eckert 2015] showed a more than 5 mmHg greater reduction in systolic office blood pressure after six months than the control group. The primary endpoint of the study therefore was reached. Also, there were significantly greater reductions in diastolic office blood pressure and systolic and diastolic home blood pressure in the intervention as compared to the control group. Thus, important secondary endpoints of the study were also reached. In contrast the decrease in ABPM daytime systolic and diastolic blood pressure in the intervention group was not significantly greater than observed in the control group which may be due to insufficient sample size, since ABPM data were not available for all study participants. Moreover, there were no differences in the evolution of life-style aspects (body mass index, amount of exercise, alcohol consumption) between the intervention and control groups. Some aspects of quality of life seemed to improve more in the intervention than in the control group.
Our study included a control group and was randomised. Our study was conducted in standard outpatient clinics, to assess whether a multisession hypertension education programme can be performed in standard German healthcare infrastructure where resources are limited.
Hypertension education programmes have been developed to increase awareness, treatment and control of hypertension and to improve adherence. For example, in the eighties of the last century hypertension awareness was less than 50 %, thus also treatment and control rates were unacceptably low [Heinemann 1998]. Several decades ago Canada developed the Canadian Hypertension Education Programme [Feldman 2008]. This programme was designed for both medical staff and patients. Within one decade, awareness, treatment and control of hypertension could be improved in Canada [McAlister 2009].
From 1990 on several patient-oriented hypertension education programmes have been promoted. Danzer and coworkers initiated a hypertension education programme at the University of Erlangen and included more than 100 patients [Danzer 2000]. The programme consisted of eight training units, 90 minutes each. At entry and after six months office blood pressure, home blood pressure, weight, physical activity and self-reported aspects of quality of life as well as knowledge about hypertension were assessed. The design of this study was similar to the present study, however in the study by Danzer et al. no control group was included. Danzer and coworkers reported reductions in office and home blood pressures, a small reduction in weight (less than 1 kg), an increase in physical activity, better self-reported quality of life and better knowledge about hypertension in the included patients.
The German health insurance companies also initiated a large health education programme for hypertensive patients [Lickvers 2005]. More than 1000 patients were included. The programme consisted of telephone advice by medical staff with the emphasis on lifestyle modification and blood pressure home measurements. All patients also received written educational material and an automatic blood pressure sphygmomanometer. After about 16 months, blood pressure decreased significantly, body mass index decreased slightly (by 0.5 kg/m2 only in obese patients) and physical activity, lipid profile and knowledge about hypertension appeared to improve. Again, there was no control group in that study.
Mühlhauser and coworkers performed a structured hypertension teaching and treatment programme in general practice [Mühlhauser 1993]. This was a controlled study, half of the outpatient clinics performed health education in four sessions, in the remaining outpatient clinics standard care was given, each clinic included 20 patients. However, out of 100 patients recruited in the intervention outpatient clinics only 46 participated in the programme. All patients were treated with antihypertensive drugs. In the participants of the hypertension education programme, there was more pronounced decrease in office blood pressure (by 5/4 mmHg) than in the control group, and more patients in the intervention group lost weight than in the control group. The follow-up was up to 18 months. Because of these findings, this hypertension education was later implemented in a total of 111 primary healthcare practices in two German districts (in western and eastern Germany) [Gruesser 1997]. The programme was well received by the physicians, a total of 466 patients were trained, and data could be analysed in 272 patients. After about six months follow-up, there was a 10/5 mmHg reduction in office blood pressure and a weight reduction by 2 kg.
An Austrian single center study documented a different approach [Kurz 2005]. Their programme focused not only on education but also on physical exercise training, sessions were held every two weeks for six months. Total follow-up was 18 months. There was no control group. Only patients on hypertensive medication were included. There was a 8/4 mmHg reduction in office blood pressure by six months along with a decrease in antihypertensive medication intensity, an increase in exercise capacity, body mass index did not change. At 18 months, blood pressure control again deteriorated, there was no long-term effect on blood pressure.
A French hypertension education programme with different workshops ("my nutrition" and "my treatment") resulted initially in better hypertension control and physical activity but on follow-up there was some weight gain and a decrease in physical activity [Mounier-Véhier 2013].
A Russian hypertension education programme (five two-hour lessons), no control group, resulted in increased hypertension awareness, a larger proportion of patients on antihypertensive medication and better knowledge about hypertension [Konrady 2001]. However, there was no significant weight loss or smoking cessation in the participants.
From these mostly encouraging results many hypertension education programmes were promoted worldwide. In Germany, as in other countries, disease management programmes were initiated for diabetes, chronic lung disease, coronary artery disease and heart failure. Part of these disease management programmes were patient education programmes. 91 German patient education programmes were reviewed [Küver 2004], 49 programmes failed the criteria at first sight, the remaining 42 programmes had significant deficiencies (e. g. lack of scientific evaluation of the efficacy, insufficient quality improvement activities).
In the last years digital health applications for smartphones have become increasingly available. These apps are designed for helping patients to achieve better blood pressure control. A recent study by Zietzer and coworkers demonstrated a reduction in systolic blood pressure by about 5 mmHg and better adherence to medication by using such a digital health application in patients with uncontrolled hypertension [Zietzer 2025].
Moreover, since about 2010, the reality of hypertension patient care has changed in many western countries. Hypertension awareness, treatment and control are generally higher than around 2000 [Neuhauser 2015]. On the other hand new hypertension guidelines promote lower target blood pressure levels [Mancia 2023, Jones 2025]. Because of the demographic evolution there is an increasing prevalence of hypertensive patients, mostly elderly patients, in western countries [GBD 2016 Risk Factors Collaborators 2017]. The German Hypertension Society has initiated a hypertension specialist programme in 2007 offering general practitioners, internists, cardiologists, nephrologists and neurologists special training courses and a degree (DHL 2017). In 2012 the German Hypertension Society developed an own hypertension education programme. To test its efficacy in the light of the changed patient care reality the present study was conducted.
A strength of this study is the randomised control group design. As in the above cited previous studies, significant reductions in office and home blood pressure could be observed by intervention. This effect was not statistically significant for 24-hours ABPM data. The observed decrease in blood pressure was not associated with measurable lifestyle changes. The patients’ knowledge on hypertension was already good at entry into the study, and there were no relevant improvements with the education programme.
The limitations of the study are the following: First, since only eight instead of 24 primary care practices could be recruited for the study, the study lacks statistical power, and the results have to be interpreted with caution. Specifically, we cannot exclude false negative results. However, we were able to find significant differences regarding blood pressure changes between the intervention and the control group. Furthermore, nearly all studies which investigated a hypertension education programme thus far had similar issues, and most of these studies did not include a control usual care group at all. The probable cause for the insufficient recruitment of primary care practices for the study was likely insufficient funding. The participating practices received no funding at all, funding provided by the German Hypertension Society just covered data collection and monitoring.
Second due to the unblinded cluster randomisation design and the preferential inclusion of untreated patients with mild hypertension, there were baseline blood pressure differences between intervention and control groups. The magnitude of blood pressure reduction by an intervention correlates with baseline blood pressure, possibly making a higher reduction in blood pressure more likely in the intervention group. However, we do not believe that this effect has significantly biased the results of this study, since patients in the intervention and control groups only had mild hypertension and the difference in baseline blood pressure was small. Moreover, analysis of variance was applied as statistical method to adjust for baseline differences.
Third it may be hypothesised that due to the unblinded cluster randomisation design differences in standard care between the participating practices could have influenced the results. We do not believe in such an effect since all participating practices adhered to the guidelides of the German Hypertension Society from 2015 for hypertension care. These guidelines included the attempt of life style changes for several months before initiating antihypertensive pharmacotherapy in patients with mild hypertension and low cardiovascular risk, a policy widely adopted in 2015 (DHL 2015).
Fourth, no information on medication was collected, therefore subgroup analysis of patients with or without antihypertensive medication cannot be performed. Moreover, no information on medication adherence can be gathered. However, mostly patients without antihypertensive medication were included in the study and any change in antihypertensive medication resulted in exclusion from the study. It may be hypothesised that the higher exclusion rate in the control group was due to increased blood pressure necessitating antihypertensive medication. However this would strengthen the efficacy of the hypertension education programme.
Fifth we can only speculate on the mechanisms that resulted in the blood pressure decrease in the intervention group: Possibly the five education sessions in small groups empowered the patients for shared decision making. A study by Deinzer and coworkers suggests that empowering shared decision making may be more effective than hypertension education alone for blood pressure management [Deinzer 2009]. It is also possible that the decrease in blood pressure in the intervention group is partly due to a Hawthorne effect [Adair 1984]. With five educational sessions within three months the patients in the intervention group received much more attention than a hypertensive patient receives in general German health care reality (on average only one or two physician visits for issues related to blood pressure per year). The observed blood pressure reduction may also be attributable to empathic and positive communication in the intervention group, as suggested by Howick and coworkers [Howick 2018]. It is possible that the effect of the presented hypertension education programme decreases over time, a longer follow-up than six months would have been necessary to examine the persistence of the blood pressure lowering effect of the hypertension education programme.
In any event the observed blood pressure reduction in patients receiving the hypertension education programme is clinically relevant. Similar or even lower pharmacotherapy-induced blood pressure reductions in patients with mild hypertension resulted in significant reductions in cardiovascular events, the relative risk reduction was approximately 20 % within five years [Sundström 2015, Diao 2012, Blood Pressure Lowering Treatment Trialists’ Collaboration 2021]. There are two published sham-intervention controlled studies of renal denervation in untreated patients with mild arterial hypertension [Azizi 2018, Böhm 2020]. In both studies the observed blood pressure reduction by renal denervation was less than 10/5 mmHg greater than in the sham-intervention groups after two months, thus in the same order than observed with the hypertension education programme. Interventional therapy for arterial hypertension cannot replace patient education, lifestyle modification and adherence and is only recommended for limited indications [Mancia 2023].
Conclusions
Given the limitations of the study, the participation in the hypertension education programme of the German Hypertension Society (MEIN BLUTDRUCK – OK!) however appeared to be associated with significant reductions of office and home blood pressure within six months for patients with mild arterial hypertension. Therefore, this hypertension education programme may be an efficient tool for hypertension management in the setting of primary health care.
|
|
Erschienen in: Diabetes, Stoffwechsel und Herz, 2026; 35 (3) Seite 139-147